Blog


Lockdown reflection: A day in the life with Sue Connell
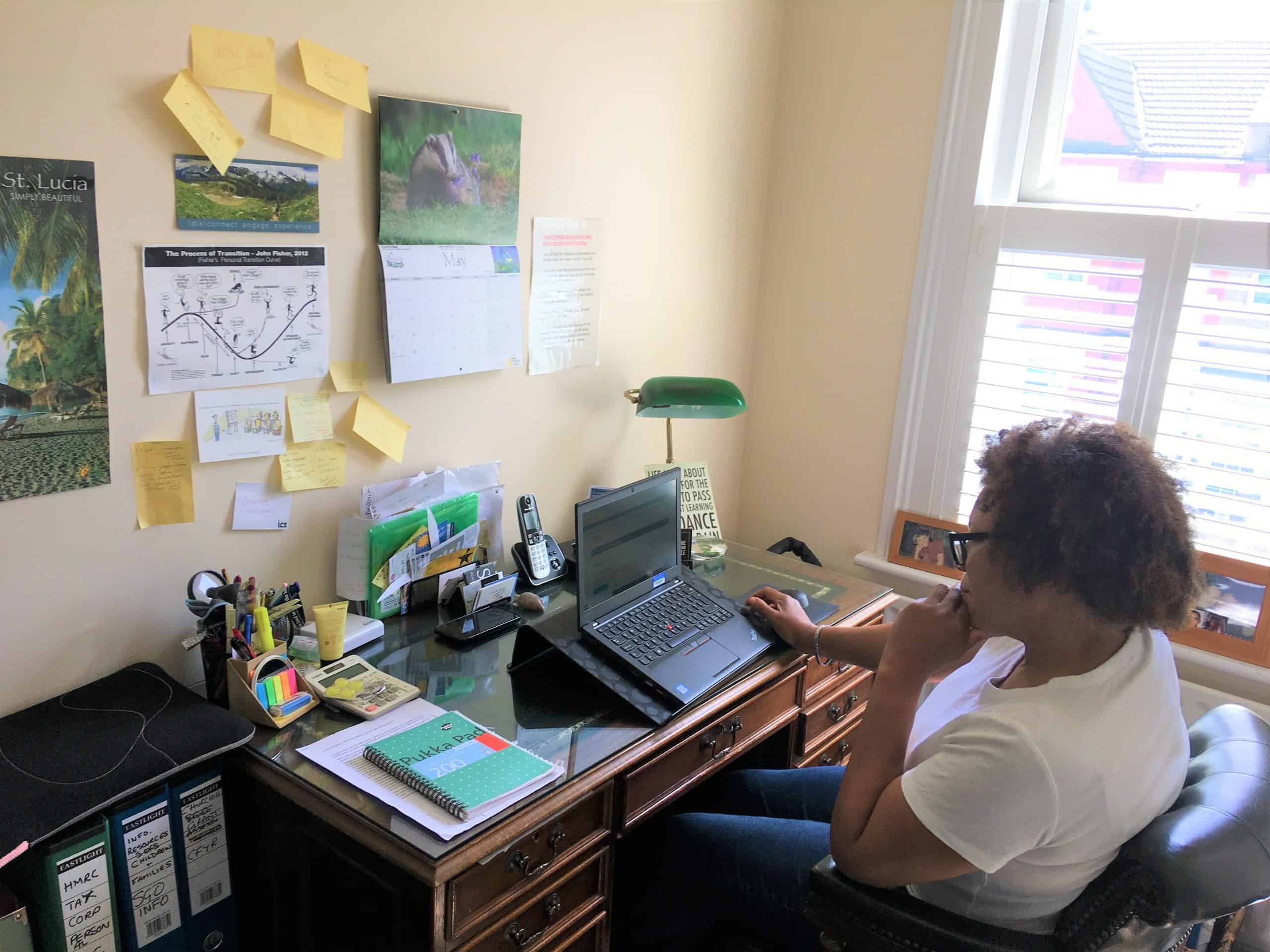
This is a guest blog by Sue Connell, Professional Practice Development Advisor at the London Borough of Wandsworth.
As an ASYE (Assessed and Supported Year of Employment) assessor, I work closely with Wandsworth’s Newly Qualified Social Workers (NQSWs) as part of the Wandsworth Children Social Care Academy (WCSCA).
The ASYE programme replaces the regular probation period and so this is a really important time for our NQSWs. Thanks to the team, the ASYE processes are continuing. The processes include: virtual panel, ASYE update meetings, the full ASYE programme of reflective supervision, support, regular reviews, appraising reflective pieces and observations.
So, how do we manage this all from home? I’m not sure how I would have coped without my little computer, but I’ve been amazed with Microsoft teams and have used Skype (for business) too.
we’re dealing with layers of risk, loss, transition and the emotions that this brings
I’m pleased to say that our reflective supervisions – where our NQSWs look at how theories apply to their work, resilience building and self-care skills, and anything else they would like to discuss – have been met with enthusiasm and I’ve been able to link in and continue to assess and support. Luckily, I have scanned the reflective resources that we use so we have a range of choices and levels of reflection.
With each meeting, I’ve come away with great ideas that NQSWs have brought to the table – they’re such fabulous team players. We’re developing virtual observations and have made a start on these. Reviews have been surprisingly easy and straight forward. I would add that the current situation brings an element of focus too: ‘getting straight to it’ as there’s so much screen time.
I am missing the impromptu visits and being able to ‘just ask’ a question.
One pattern that’s come up for the group is how busy they are, but in a different way. It’s a good reminder that we’re dealing with layers of risk, loss, transition and the emotions that this brings – I’m certainly finding that.
Florence and I facilitate Action Learning Sets, which is a sort of structured peer supervision. We will be arranging to facilitate these virtually to ensure this ongoing support at a time when it’s most needed. I am booked onto the webinar for my first bit of training on how best to adjust to the virtual style – such a learning curve!
Of course, there are challenges; the ‘togetherness’ is harder to maintain and takes that bit of extra work. I am missing the impromptu visits and being able to ‘just ask’ a question. Also, coffee time in the office is a great opportunity for team building and I’m missing that. So, we must be creative and put in that extra effort to keep connected.
Today, I will be working on my next final report. It’s a privilege to capture (and analyse) all the hard work and learning that each of our NQSWs have completed and to see them ‘fly the nest’.
… well, a cup of tea always helps too.
We have three due for panel and more coming through soon. The couple of virtual meetings later will bring a nice balance to the day. What else? … well, a cup of tea always helps too.
Tell us your social work story at stories@socialworkawards.com telling us your name, job, contact details and social care number (just so we know you’re a social worker, we will keep it private).

If you can’t go home, we will bring home to you.
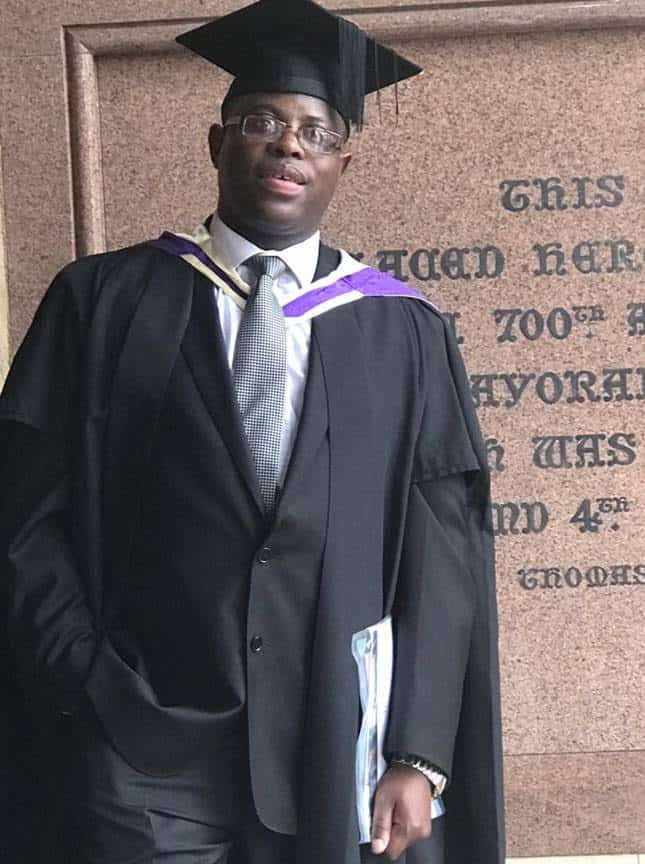
This is a guest blog by Wendy Ashton, Palliative Care Social Worker and Family Support Team Lead at Eden Valley Hospice and winner of the Making a Difference Social Worker of the Year Award 2018.
As a palliative care social worker in a Hospice, Covid 19 has really challenged my ethics, morals and ways I practice – hopefully for the better in the long term.
I work in a small Hospice that covers a vast rural community as a full time Palliative Care Social Worker and Family Support Team Lead. I work with people at end of life who have complex needs and aim to make the time that people have left as happy and content as possible. A large part of my role involves working with families and friends as well as clients.
Technology for good
Often, a patient is too unwell to return home and chooses to die at the Hospice. A last wish is often to see home for one last time, and we can arrange this with a carer and transport for an hour at home. It is tricky to organise, but it is worth it when you see the joy on that patient’s face when they return after seeing home for the last time.
The High School Musical Song ‘We’re all in this together’ springs to mind frequently
Unfortunately, this was not an achievable goal with lockdown. However, I am not one to give up so, after speaking to the patient’s husband, we set up for him to video the house room by room – including the cats in it too.
The patient’s husband did this and, after a bit of IT help, we downloaded 2 short videos onto a laptop that we left in the patient’s room. She watched the clips with animation, showing staff her beautiful home that she was so proud of.
The cats (too feral to visit apparently – we had suggested) also made an appearance and the patient was ecstatic to see them. She watched those clips daily for a couple of weeks before she became too unwell to watch. A truly positive and happy outcome. If you can’t go home, we will bring home to you.
Supporting families
On another day, a patient was dying and was Covid positive. One family member was allowed to see her – with full PPE on – but others were upset they could not say goodbye too. I set up a WhatsApp call with the family so they could all say their goodbyes to her.
Although the patient was unresponsive, hearing is the last sense to go – we truly believe she died knowing that all her loved ones said goodbye before she died.
we have given lots of virtual hugs and hands on shoulders to comfort
We also had volunteers knitting hearts for the Hospice; the patient kept one and her family were sent matching ones that were bagged for the quarantine period prior to sending out.
Keeping connected
As a social worker I have used Facetime and WhatsApp to connect family and friends. We’ve had family/MDT meetings in the gardens sat 2 metres apart, and we have given lots of virtual hugs and hands on shoulders to comfort. It has been difficult at times trying to make a difference at end of life, but I feel we have been successful within our restrictions and limits.
I’ve had heart-breaking moments when I could not initiate change. A lady in her 50s was troubled constantly in her last week of life. When I asked what was wrong and could if I help, she told me that she was struggling to decide which 10 people could go to her funeral. How on earth can you answer that? I could not do anything except listen – often that helps.
A good quality of life is so important even if it is only for a day or two. I love my job and hope that we can continue to work to achieve dreams and happiness at end of life with our clients and families. I know I will keep on trying.
I could not do anything except listen – often that helps
Social workers play such a valuable role at end of life for both clients and families and friends.
Tell us your social work story at stories@socialworkawards.com telling us your name, job, contact details and social care number (just so we know you’re a social worker, we will keep it private).
Lockdown diaries : A day in life with Mary Scarlett
This is a guest blog by Mary Scarlett, Safeguarding (Schools) Lead Training and Development Officer at Wandsworth Children’s Social Care Academy
Will social distancing be our new working norm?
When I left the office on 10th March, I had no idea of the roller-coaster of thoughts and emotions I was sleepwalking into, and that I would finally hit a “brick wall” at about the fourth week.
At the beginning, I thought it was a bit of a novelty, even though working from home and using virtual platforms has always been a significant feature of my Social Work life.
Initially, I welcomed the team daily Keeping in Touch (KIT) meetings using the MS Teams platform. I willingly attended every day even though I worked 3 days a week. That soon wore off, appearing to me as no longer being a choice, but a necessity.
I had no idea of the roller-coaster of thoughts and emotions I was sleepwalking into
In what seemed to be a wave of anxiety, I began to think that if I did not attend and take responsibility for my understanding and learning, I would always be behind the curve playing catch up.
It was like a runaway train, every man for himself justifying the adaptability of their roles in these unprecedented circumstances.
What also became apparent to me, was the different group dynamics that played out in the team virtual meetings; this had me thinking about the four group stages: forming, storming, norming and performing.
Whilst I acknowledged we were an established group; in reality we were a group trying to operate and communicate in very different situational circumstances which seemed to be working for some and not for others.
It was like a runaway train, every man for himself
It appeared to be “business as usual,” but in my mind it couldn’t be – these were unprecedented times, things were moving and changing very fast, both in our personal and working lives.
Technology had become our new BFF as well as an appendage which you wanted to cut off when it did not work, only adding to the anxiety and stress.
The level of information that was being shared and meetings being convened felt like “white noise”; it was not relevant to my role and it felt impossible to retain it all.
It appeared to be “business as usual,” but in my mind it couldn’t be
I soon mentally and emotionally withdrew from the process, choosing to be visible or invisible during the team meetings depending on how I was feeling that morning, and it seemed to me no-one noticed.
What I have taken away from this lockdown period is, as agents of change, how much do we really hear, are we even listening, and how much do we really see, or notice, when we’re looking at each other on a screen?
For some it’s may be the new way forward for practice but, for me, there is the danger, is it taking us down a path of permanent social distancing?
Share your social work story at stories@socialworkawards.com telling us your name, job, contact details and social care number (just so we know you’re a social worker, we will keep it private).
Power, Trust and Race
This is a guest blog by Eddie Dube, Social Worker at Somerset County Council
Throughout my career as a social worker, I have worked in situations where trust is weak or entirely absent. This could be due to negative past experiences at the hands of social services such as perceived over-intrusion, a negative representation of social services in the media, or historic abuse of power by the powerful.
Mistrust can also be rooted in history, such as the prejudices and injustices experienced by people of colour.
History matters – it’s part of the bigger picture that shapes who we are. My lecturer, Collin Rones, used to remind us to always look at that bigger picture and avoid focusing solely on our own individual perspective, which can make us see only what we want to see and reinforce what we already believe.
History matters – it’s part of the bigger picture that shapes who we are.
It is that bigger picture that I want us to look at to help us understand what has been happening lately: the Covid-19 pandemic and the murder of George Floyd by police in America.
A recent report found that Black, Asian and other minority ethnics (BAME – a term I dislike for the way it stereotypes a hugely varied group of people) have been disproportionally affected by Covid-19, with death rates higher among people of black and Asian origin than any other ethnic group. A Public Health England report pointed out that “racism and discrimination suffered by Britain`s black, Asian and minority ethnic people contributed to high death rates from Covid-19 in those communities”.
According to the Guardian, the report further states “racism and discrimination experienced by BAME key workers is a root cause affecting health and exposure risk. For BAME communities, lack of trust of NHS services resulted in reluctance to seek care”. Why is there a lack of trust in NHS services by these communities, when quite a large percentage work for the NHS and mostly on the frontline? Is the report alluding to racial discrimination by the NHS, either in the form of institutional or organisational racism?
What is racism, anyway? For black people, it traces back to the slave trade, which justified its cruelties with a mixture of pseudo-science and negative stereotypes. The dehumanisation suffered by black people during slave trade is part of our shared history and has unavoidably shaped our modern world.
But something being normal does not make it healthy, or right, nor does it mean we have to accept it.
It might be unnoticeable to some, but it’s there, passed down through generations like a family heirloom, or like a statue on a street which we don’t really notice because it’s always been there. It feels normal to us that it’s there.
But something being normal does not make it healthy, or right, nor does it mean we have to accept it. One of the most striking features of our shared history of racial discrimination was how normal it was – almost everyone thought this way, and black people were expected to accept it. These social norms have always been shaped by those who have power and want to keep it – it was the case during the slave trade, it was the case after the emancipation, and is still the case now.
What made George Floyd different was that we saw him.
Recent news reveals that the slave trade is still alive and well and is closer to home than we all care to admit. Many of us are unknowingly wearing clothes or using technology that are the end products of a supply chain which relies on exploitation and/or child labour.
Modern slavery surrounds us, and its victims live invisibly among us – serving our food, picking our crops, and working in factories. From the outside, they seem to have normal jobs, but behind closed doors they are exploited for personal gain, forced into debt, and threatened with violence. The old slave owner mentality never went away, it just went into hiding.
What made George Floyd different was that we saw him. The death of a man, captured on video in real time, in the hands of someone who should be a protector was a massive wake up call for us all. The killing of George Floyd refocused the spotlight on the power of the police – why are black people so over-represented in the justice system, prisons, stop and search, not to mention Covid deaths and unemployment?
The numbers might have something to do with the way black people have been portrayed: as animals, uncontrollable, criminally minded and dangerous.
As long as we are defined by our race and ethnicity, inequality and injustice will continue.
Because of this, more black people are handcuffed by the police at the very first instance. The negative portrayal of black people has fractured our society, creating an ‘us and them’ mentality which thrives on mistrust.
What can we do about all of this? Laws and legislation which make discrimination illegal will take us part of the way but will depend on political willingness to apply them. Dr Martin Luther King Jnr said; “The law cannot change the heart but can restrain the heartless”, so we need more than just the law – we need systems that promote social justice and humanity, and we need to start challenging ideas which keep us in bondage. As long as we are defined by our race and ethnicity, inequality and injustice will continue.
A new social contract is needed to build trust between black people, the state and its systems. State institutions need to start to build trusting relationships that eradicate systematic segregation and discrimination, and this needs to happen quickly.
The Ethical Framework for Health and Social Care is a very good tool that can be used to rebuild trust across the system. It can be used by the police force, health delivery systems, employers and even policy makers. The framework looks at the big picture, which makes it particularly relevant to the current climate, not just in light of Covid-19.
The Ethical Framework for Health & Social Care
By the Department of Health & Social Care
1. Respect
Recognise that every person and their human rights, personal choices, safety and dignity matters.
2. Reasonableness
Ensure that decisions are rational, fair, practical, and grounded in appropriate processes, available evidence and a clear justification.
3. Minimising Harm
Strive to reduce the amount of physical, psychological, social and economic harm that the outbreak might cause to individuals and communities. In turn, ensure that individual organisations and society as a whole cope with and recover from it to their best ability.
4. Inclusiveness
Ensure that people are given a fair opportunity to understand situations, be included in decisions that affect them, and offer their views and challenge. In turn, decisions and actions should aim to minimise inequalities as much as possible.
5. Accountability
Hold people, and ourselves, to account for how and which decisions are made. In turn, this requires being transparent about why decisions are made and who is responsible for making and communicating them.
6. Flexibility
Be responsive, able, and willing to adapt when faced with changed or new circumstances. It is vital that this principle is applied to the health and care workforce and wider sector, to facilitate agile and collaborative working.
7. Proportionality Provide support that is proportional to needs and abilities of people, communities and staff, and the benefits and risks that are identified through decision making processes.
8. Community Commit to get through the outbreak together by supporting one another and strengthening our communities to the best of our ability
For full advice and guidance under these principles, visit:
Share your social work story at stories@socialworkawards.com telling us your name, job, contact details and social care number (just so we know you’re a social worker, we will keep it private).Read Less

‘Shifting sands and thinking on your feet’: a day in the life of an AMHP
This is a guest blog by Frances Folkard, an Approved Mental Health Professional (AMHP).
Our days are mostly about arranging and conducting Mental Health Act Assessments. Any AMHP will tell you “a day” is never the same as any other.
Conducting a Mental Health Act Assessment is like setting off on an expedition. The AMHP thinks: “I am trained for this, I have some tools, I am as prepared as I can be. I have gathered the troops and 2 doctors, I have a destination sorted, the bed and the possibility of assistance, with an ambulance if needed” and off you set.
Conducting a Mental Health Act Assessment is like setting off on an expedition.
But what you don’t know is: “how is this going to end, or when?” – so many dilemmas & variables ahead, ‘shifting sands’, thinking on your feet; unanticipated things presenting.
And you hope for some good luck, because you’ll need it!
Let me tell you about a situation I was recently involved in. We received a referral for a 28-year-old woman who lives alone – we will call her Kiri. She has a diagnosis of bi-polar disorder, has cardiac problems and has a mild Learning Disability.
Kiri started becoming unwell a few weeks ago and is now beyond treatment in the community. The referral tells me she “is paranoid, suspicious & aggressive – believes food is poisoned and has stopped eating”. Kiri rings her Mother constantly throughout the day.
Was there need for a Mental Health Act Assessment? Yes. I emailed doctors, none were available that day.
Thursday. One Psychiatrist could do 5pm. I finally found another who could do that time too.
I met one Psychiatrist outside the woman’s home. We waited. I texted the other, she was delayed getting PPE. I rang and asked if she could get some for us and the patient – a kind woman, she already had. She arrived. The patient’s mother said she has a key and could let us in. I reserved that as a fallback preferring to knock and see if Kiri would let us in herself.
We could hear loud talking. We knocked and knocked, called through the letter box, telephoned. No reply.
I rang the patient’s mother, she came, opened the door with her key and disappeared again. We entered the hall and said hello, heading towards the stairs thinking she was upstairs. But no, Kiri was in a room to the left back of house, sitting on sofa with cat on her lap. She jumped up, slammed the door, and shouted at us to get out. We explained why we were there and wanted to talk to her – “No, get out. You’re Nurses, you’ve lied to me, go away”.
Dr A has a soft kind voice and told Kiri she was a doctor. She became aggressive in manner, shouted at us to leave and said she knew us very well – we had not met her before. She told us to go or she would call the Police. We said to call the Police and tell them we are here. She rang 999. We could hear her giving her address. We ask: “Please tell them Dr A is here”.
I went outside and rang 101; I told Police that Kiri was on a 999 call to them and that we were in attendance for a Mental Health Act Assessment. I asked them to link both calls on their system. We told her we were leaving and left.
The Psychiatrists felt they had enough to write a joint medication recommendation. We sat in Dr A’s car. We then heard Kiri’s voice shouting on the street saying that her father had raped her. Dr A approached the patient’s gate smiling and said: “I am Dr A, we have not met before, I am very pleased to meet you”. Kiri shouted back: “you are my father”. Dr A, from Nigeria, said: “look at the colour of my skin, do you really think I am your father?” Kiri replied: “you are a cross dresser, you are a fake, you are my father” and went inside.
The exchange confirmed our assessment. Back to the car to continue. A Police car then arrived. It was a PC responding to Kiri’s call to Police. He knocked on the door, but she did not reply. I asked for his mobile number as I might need his help when the ambulance arrived – Kiri’s mother told me she put up a lot of resistance last time.
lots of people in the terraced houses on both sides of the street came out and clapped for the NHS, but Kiri did not emerge.
He gave me his number. Papers were completed at 19:15. I rang SWAS (South Western Ambulance Service) and requested an ambulance. They said they would try to attend within the hour. The Psychiatrists left.
The Police officer stayed on the street. At 20:00 lots of people in the terraced houses on both sides of the street came out and clapped for the NHS, but Kiri did not emerge. I rang the ambulance for an ETA – it had not yet been allocated. I was told that one was on its way to us at 19:50, but it had been diverted to a cardiac patient.
At 20:10 a triage doctor from SWAS rang me and asked if a PTV (patient transport vehicle) would suffice. I explained that Kiri has a cardiac condition and I wanted a paramedic crew in attendance in case anything happened on the way, short journey as it was.
From the moment I signed the AMHP application form the patient was in my custody.
I stood there thinking not only: “what if she doesn’t answer the door and let us in?”, but: “what if she locks the door from the inside so her mother’s key won’t be able to open it from outside?”.
Would we have to go to court & get a S135(2) warrant? Oh no.
The PC and I shared concerns and all kinds of anticipated problems.
At 20:45 the ambulance arrived. A 2-person crew. A woman driving & a tall dark-haired young man to approach the patient. He geared up. We agreed the PC would go in first, me behind him. I was going to tell Kiri that the doctors and I are concerned she is not well and that we think she needs a period of assessment on X Ward etc. I would not tell her she was detained, for fear of increasing her stress or affecting her cardiac condition.
The PC and I shared concerns and all kinds of anticipated problems.
We knocked on the door. No response. The PC talked through door, all quiet. I rang the patient’s mother – she had been parked nearby; she came and gave me her key, then she ran off again (fortunately she owned the house).
Phew! Kiri had not locked the door from the inside and left the key in the lock. We got in.
Kiri was standing on the second from bottom step on the stairs. She looked cross. I explained what was going on and ended saying: “so Elliott has come with an ambulance to take you there”.
She took one look at Elliott, the male paramedic, and her face broke into a wide beam. She trotted towards him in bare feet, not interested in finding slippers or shoes. She boarded the ambulance without difficulty.
At that point she looked like a young girl, a hint of her learning difficulty becoming apparent.
And that was the luck. Had it been Elliott driving and his female colleague approaching the patient – it could have been a completely different set of circumstances.
Kiri was admitted to hospital safely.
Share your social work story at stories@socialworkawards.com telling us your name, job, contact details and social care number (just so we know you’re a social worker, we will keep it private).

A Plumber’s bag and ten extra minutes
I will always remember my consultant social worker comparing social workers to plumbers. ‘Just like a plumber can’t do their job without their plumber’s bag, said Jo, ‘a social worker can’t do their job without their social work toolkit’.
Armed with knowledge and skill, they also need various tools… to get the job done.
A plumber needs a range of tools and equipment to successfully change that pipework, install your new sink or unblock your washing machine. Armed with knowledge and skill, they also need various tools such as a pipe wrench, faucet key and plumber’s tape to get the job done.
Just like our social work training equips us with the theoretical knowledge and skill to work as social care professionals, social workers too need their own toolkit bags. Taking a few moments to reflect that I was indeed working in a social work team and not a building site, it all clicked into place when I started to build my own social work tool bag. No one can tell you what to put in your tool bag, it’s your bag. Some may have support plans, a pen and a consent form. I had colouring pens, an A1 size flip chart pad and Sharpies.
I was privileged to work in a new, social work-led mental health, forensic and substance misuse team for my first year as a qualified social worker. In this team we worked with people and change; we would work with resistance, distress and ambivalence.
We ran social work and peer-led groups sessions weekly and linked with our local community to offer opportunities to adults living with mental illness. We also supported people with enduring mental illness into voluntary work and some into paid employment – it was the best year a newly qualified social worker could ask for.
An alternative approach
In this team, I was introduced to an alternative (or creative) approach to social work under the tutorage of my assessed and support year in employment (ASYE) practice educator Lawrence Taylor.
He always helped me try and see and feel what it would be like to be in the shoes of the people I work with. How would I want to be treated or assessed?
I recall once time working with Sam, a 18-year-old adult with autism, obsessive compulsive disorder and bulimia. Sam rarely spoke but when he did, it was only about philosophy or space. Sam preferred texting, emailing or drawing, but again it was mostly around his areas of interest.
I opted one day to bring in my brand new pack of Sharpies and an A1 flipchart pad; we had a semi directed session about the future and goals and each took it in turns to ‘share and tell’ out picture with a narrative.
At the end of a 60 minute assessment, Sam has drawn what his worries were, his fears, his plans for the next six months, his five-year goal and what he wanted to achieve from his social worker.
Sam has drawn what his worries were, his fears, his plans for the next six months, his five-year goal
They were all pictures, but Sam was empowered to tell me in his narrative whilst I quickly jotted down these important points on my pad. When reflecting back to me what each picture meant to him, we were able to hold a short, but meaningful conversation about what would evenly lead to his support plan.
I was able to complete a detailed assessment of his needs, wishes and goals and we worked closely for the next few weeks towards getting Sam back to college. The A1 pad and Sharpies were now my wrench in my social work tool bag. As the months and years pass, I’ve added small figurines, toy cars, characters from the film Inside Out, MoodCards and a pair of magnets.
Time to plan
Fast forwording four years to 2020, I had moved on from my social care mental wellbeing team into a seconded Approved Mental Health Professional (AMHP) Hub. Along with this came the more legalist approach of social work assessment in the form of Mental Health Act Assessments.
I feared my ‘Plumber’s bag’ would be out of action for some time, having to coordinate the detailed assessment undertaken with doctors under the Mental Health Act and facilitate the safe admission or home care of individuals in a mental health crisis.
As Covid-19 restrictions came into place, the AMHP hub continued to operate 24 hours a day, seven days a week. As other friends and colleagues were working from home, reviewing individual and families remotely, AMHPs were still very much out conducting face-to-face assessment (or interviews).
The county I serve is a mixture of rural and urban, the drives often require a scenic and traffic heavy route through the South Downs. During the Covid-19 restrictions with less traffic on the road, I found myself getting to places with extra time to spare (which in reality meant on time, as a social worker, I’ve always been working 10-15 minutes late since starting this career).
Having this extra time meant that I had opportunities to plan for my intervention a little more.
Alternatives to talking
I recall one day planning to assess Betty, who was in hospital under section 2 of the Mental Health Act 1983. Her consultant has asked for an AMHP and second doctor to assess to consider if Betty should now become subject to the provision under section 3, as she required a longer period of treatment.
Betty was 40-years-old. I was fortunate to have assessed her the previous month, so knew a little about Betty’s history. She was assessed under the Mental Health Act and detained under section 2 following a lapse of her illness and what is being described as selective mutism. She would not talk.
When I assessed Betty the previous month, I tried a variety of different approaches including writing, drawing and eventually using my laptop to type a variety of closed and open questions to which Betty was able to respond – this indicated to me that she was able to read and felt more comfortable responding to written questions / using alternative communication methods.
Whilst waiting for my independent section 12 approved doctor, I was thinking about how I could be as inclusive as possible to Betty in her assessment rather than reply on my laptop. The Code of Practice for the Mental Health Act chapter 14.42 directs AMHP is to consider alternative communication methods to increase participation of the assessment and to break down barriers to maximise the person’s involvement in the assessment.
Rekindling creativity
I decided to have a look in my Plumber’s bag in the boot of my car. I found my MoodCards; I selected a variety of moods and emotions from the pack (which you can see from the picture range from positive moods/emotions such as happy, hopeful, satisfied to negative moods/emotions such as sad, worried, depressed et cetera).
At the beginning of the assessment MoodCards were introduced to Betty along with the purpose of the cards. I made sure they were in reaching distance from Betty and I also made no further reference of drew any attention to them for the rest of the assessment (as a means of using them as a semi-directed prop).
After approximately 30 minutes, and during a protracted period of silence, Betty reached for the blue ‘Sad’ card and said: “I feel sad,”. She then replaced this and picked up the orange anxious card and Betty said: “I feel anxious too”. These two cards open a meaningful, but limited dialogue with Betty talking further about the feeling of unease and worry on the ward.
An extra ten minutes
You may not see from the picture, but unease and worry were not emotions or mood that were on these cards. We had a small conversation and the doctor made some suggestions about medication which could reduce her feelings of anxiety.
By unpicking her emotions, I was able to glean an understanding of her current thinking pattern without the need for a protracted and detailed dialogue
This intervention worked particularly well at encouraging Betty to talk about her emotions, which had been unsuccessful in previous standard assessment approaches. By unpicking her emotions, I was able to glean an understanding of her current thinking pattern without the need for a protracted and detailed dialogue, which Betty has previously found difficult.
Whilst Covid-19 has impacted a range of services which has been awful and distressing for many, I have found having those extra ten minutes to plan for my intervention has been an opportunity for me to rekindle creative approaches to my practice as a social worker and an as AMHP.